A study published in Intelligent Oncology presents PSIDMViT – a diffusion model that integrates physical priors, spatial priors, and a Vision Transformer – delivering Monte Carlo (MC)–level dose accuracy for CyberKnife radiotherapy in just 18 minutes per patient, a 3.5‑fold speedup over GPU‑accelerated MC.
Background
MC dose calculation is the gold standard for CyberKnife stereotactic body radiotherapy, but its stochastic particle transport demands ~1 hour per patient, severely limiting routine clinical use. The widely adopted finite‑size pencil beam (FSPB) algorithm is fast, yet it systematically underestimates doses in heterogeneous tissues (lung, liver) – particularly under stringent 1%/1mm criteria. Balancing dosimetric accuracy with computational efficiency remains a critical unmet need.
Study Overview
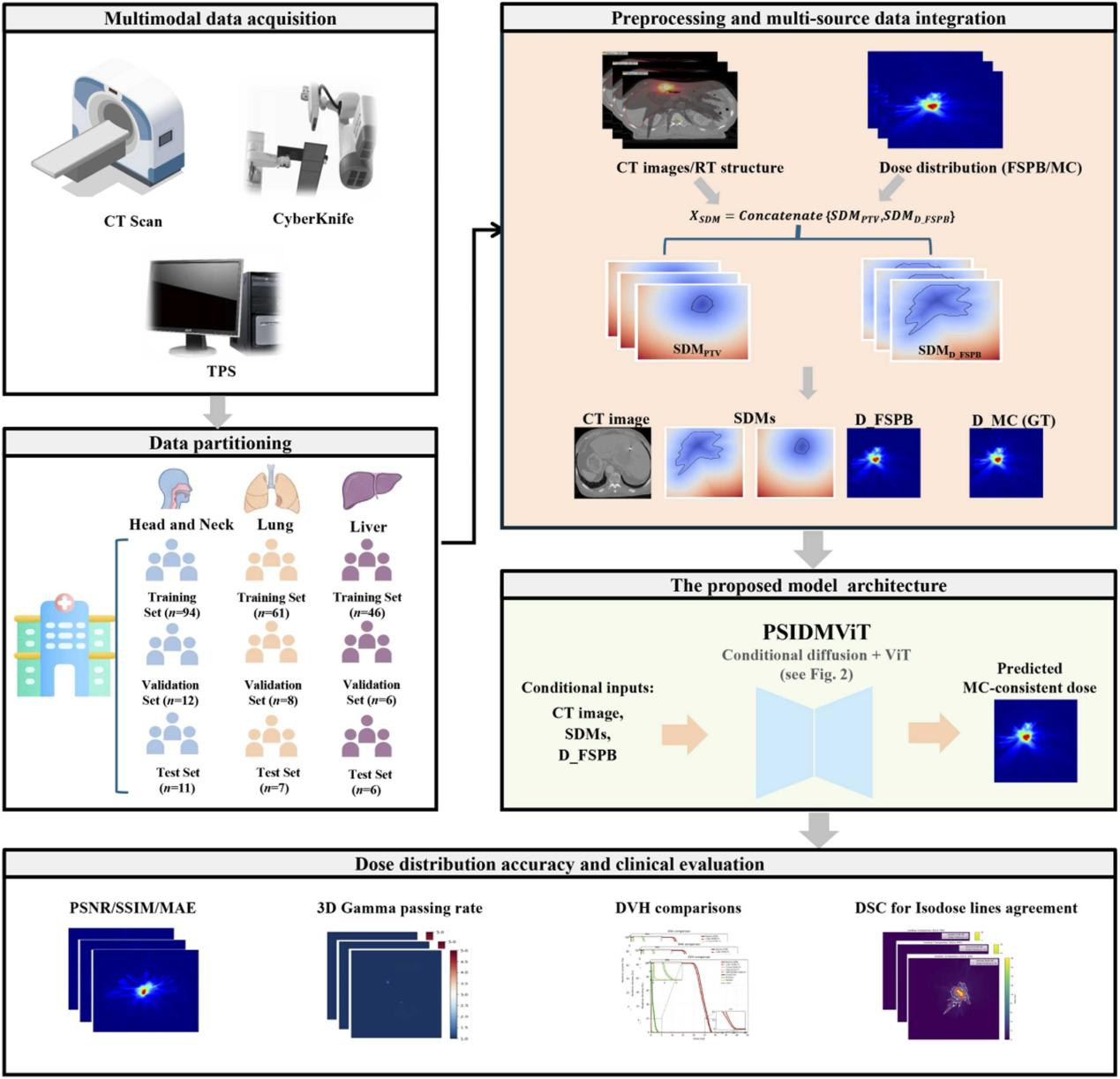
The researchers developed PSIDMViT, a conditional diffusion model that uses FSPB dose distributions as physical priors and multi‑channel signed distance maps (SDMs) – derived from the PTV and FSPB dose masks – as spatial priors, combined with planning CT images for anatomical context. A Vision Transformer module embedded at the U‑Net bottleneck captures long‑range scatter effects. The model iteratively refines FSPB doses over 1000 denoising steps to match MC ground truth. The study enrolled 251 patients (117 head & neck, 76 lung, 58 liver) treated with CyberKnife, split 8:1:1 for training/validation/testing. GPU‑accelerated MC (1% statistical uncertainty) served as the reference.
Key Findings
High dosimetric fidelity – Under the global 1%/1mm/10% Gamma criterion, PSIDMViT achieved passing rates of 98.000% ± 2.500% (head & neck), 94.000% ± 1.500% (lung), and 95.000% ± 1.800% (liver) – an absolute improvement of >10 percentage points over the best baseline (PIDM) in heterogeneous sites.
Clinical validation – Dice coefficients for isodose contours exceeded 0.972 across all sites, and dose‑volume histograms closely matched MC references, successfully correcting FSPB’s systematic underestimation in organs at risk (e.g., aorta, trachea).
Computational breakthrough – Average inference time was 18 minutes – a 3.5‑fold acceleration over GPU‑MC (~1 hour) – with deterministic, noise‑free outputs.
Ablation insights – Stepwise introduction of SDM spatial priors and the ViT module produced statistically significant gains (Wilcoxon, p<0.05), confirming that the diffusion mechanism, continuous spatial constraints, and global attention each contribute uniquely to the performance leap.
PSIDMViT offers a clinically viable pathway for offline secondary dose verification, achieving MC‑equivalent accuracy without the prohibitive computation time. With further acceleration, it may eventually support online adaptive workflows.
Full article available on ScienceDirect:
https://doi.org/10.1016/j.intonc.2026.100067
Contact Information for Intelligent Oncology:
LinkedIn: @IntelligentOncology
X: @IntelligentOnco
Facebook: @intelligentoncology
Email Address: editorialoffice@intelligent-oncology.net
Official Website: https://www.sciencedirect.com/journal/intelligent-oncology
Submission Link: https://www2.cloud.editorialmanager.com/intonc/default2.aspx